

To cite this article
Walton, L. R., Seitz, H. H., & Ragsdale, K. (2012). Strategic use of YouTube during a national public health crisis: The CDC’s response to the 2009 H1N1 flu epidemic. Case Studies in Strategic Communication, 1, article 3. Available online: http://cssc.uscannenberg.org/v1/v1art3
Access the PDF version of this article
Strategic Use of YouTube
During a National Public Health Crisis:
The CDC’s Response to the 2009 H1N1 Flu Epidemic
Laura Richardson Walton
Mississippi State University
Holli H. Seitz
University of Pennsylvania
Kathleen Ragsdale
Mississippi State University
Abstract
The emergence of the 2009 H1N1 influenza epidemic produced a number of unique communication challenges for the Centers for Disease Control and Prevention (CDC). Part of the CDC’s response to these challenges included the strategic use of video posted to YouTube to address the public’s need for information in a timely and accessible way. This case study includes an examination of the context in which this communication response took place, an overview of the research and strategy development that informed the strategic communication, and an evaluation of the response.
Keywords: health communication; social media; public relations; strategic communication; emergency and risk management
Introduction
In mid-April 2009, a new strain of influenza (later termed the 2009 H1N1 flu) was identified in a 10-year-old California patient. The unique strain of influenza virus initially emerged in Mexico and began to spread rapidly throughout the United States (U.S.). By the end of April, the Centers for Disease Control and Prevention (CDC) was certain a national public health emergency existed.[1] As the H1N1 epidemic emerged, the CDC activated the Emergency Operation Center and the Joint Information Center, which is the hub of CDC strategic communication during national health emergencies. Years of strategic planning and emergency exercises in preparation for a global influenza pandemic were paying off, but there was one element of this epidemic that the CDC could not have been predicted: the dynamic online communication environment in which this major public health event would take place.
At the time of the 2009 H1N1 outbreak, Twitter was emerging as a key online medium for exchanging brief news and information, while Facebook had more than 200 million users (Zuckerberg, 2009). Earlier that same year, YouTube had 100 million viewers and an estimated 76.8 percent of U.S. Internet users were online video users (comScore, Inc., 2009). According to 2011 data, the average YouTube user is female and between the ages of 25 and 54 years old (Ignite Social Media, 2012), making the online video-sharing platform an ideal tactic for targeting caregivers of both small children and the elderly – the two populations most at risk for complications from the H1N1 virus. The increasing importance of social media during disasters and emergencies was confirmed by the American Red Cross in its 2010 study, indicating 82 percent of participants (N=1,058) utilize social media weekly with nearly half of respondents (48%) participating daily (American Red Cross, 2010). Interestingly, only 1 in 6 participants reported using social media to obtain information about a disaster or emergency, but nearly half of participants utilizing social media daily indicated they would share disaster or emergency information via social media channels (American Red Cross, 2010).
Due to the rapid expansion in popularity of these online communication channels, social media specialists at CDC were brought into the 2009 H1N1 response to create a communication strategy for social media channels that would complement traditional media strategies. Although the social media plan would eventually involve a heavy presence on Facebook and Twitter, YouTube was used early in the CDC’s response to provide timely, accurate, and credible health messages via social media. Indeed, one of the first 2009 H1N1 videos released by the CDC garnered 2.1 million views on YouTube.
Background
As a federal agency within the U.S. Department of Health and Human Services, the CDC employs more than 15,000 staff and is the agency primarily responsible for public health (CDC, 2010a). The response to the 2009 H1N1 outbreak was likely influenced by agency dynamics in the years and months leading up to the outbreak. Prior to the event, the CDC’s emergency communication function had been tested as the agency responded to an outbreak of Severe Acute Respiratory Syndrome (SARS) in 2003, public health issues related to Hurricane Katrina in 2005, and containment of highly drug-resistant tuberculosis in 2007. During the 2009 H1N1 event, the CDC was headed by an interim director, Richard Besser, M.D., whose considerable expertise in managing national emergencies had been honed during his years as the Director of the Coordinating Office for Terrorism Preparedness and Emergency Response (COTPER).[2]
Within the U.S., the first wave of H1N1 began in April 2009, peaked during May and June of that year, and began to decline in early August. At that point in the epidemic, 477 deaths had been linked to H1N1, including 36 children under the age of 18. The second wave of H1N1 peaked in October 2009, during which 49 states reported H1N1 cases in one week alone. October also marked the launch of the national H1N1 vaccination campaign, which was designed to encourage stakeholders to take all necessary steps to protect themselves from this highly contagious and potentially deadly strain of influenza. The risk communication efforts continued into January 2010 and culminated with President Obama declaring January 10-16, 2010, to be “National Influenza Vaccination Week,” a designation that drew considerable attention to the continued necessity of precautionary measures against H1N1 (CDC, 2010c).
The CDC’s Formative Research
At the time of the 2009 H1N1 outbreak, CDC had been preparing for the possibility of an epidemic influenza event for several years. This preparation included the development of a series of manuals for crisis and emergency risk communication, with one specifically designed to address an epidemic influenza event (Reynolds, 2007). In addition, CDC had recently completed a planned emergency hurricane response exercise, during which―for the first time―social media had been incorporated as part of the CDC’s official emergency response structure.
While the CDC’s H1N1 response plan was clear, the social media structure was less well-developed. The constantly evolving nature of social media technologies provides both considerable opportunities and considerable planning challenges for public health practitioners. During the early stages of the expansion of social media, the CDC recognized that posting public health-related videos on YouTube would makes it possible for the Center to disseminate complex health messages—such as how to properly wash one’s hands to prevent the spread of infectious diseases—that cannot be conveyed easily through print media. Although the CDC had established a YouTube channel to broadcast health-related videos prior to implementing its H1N1 response plan, the Center had not yet established a presence on Facebook and had limited experience with Twitter. Because the CDC recognized that H1N1-related public health messages were necessarily going to be extremely complex, the Center’s communication specialists decided to deliver online video health messages via YouTube as a complement to traditional media strategies in order to expand the dissemination of H1N1 prevention/treatment messages to as broad an audience as possible.
In addition to developing new social media channels, the CDC also had to quickly develop H1N1 flu messages that were appropriate for the channels. Prior to the H1N1 epidemic, CDC had invested time and resources into the development of general epidemic flu messages and seasonal flu messages for use in social media. With the onset of the H1N1 epidemic, the CDC was able to adapt these pre-existing messages for use in the H1N1 social media campaign. For example, the CDC regularly conducts focus groups with target audiences to test seasonal influenza messages (which typically target vaccination), and was able to draw on those findings when crafting H1N1 messages. In addition to the ongoing research on seasonal flu messages, the CDC also conducted a thorough evaluation of epidemic flu messages in 2005. This research included focus groups with general audiences and healthcare providers in four regions of the U.S. (Janssen, Tardif, Landry, & Warner, 2006). This research contributed to the development of key messages for the public about epidemic flu—messages that could be adapted for social media during the H1N1 flu outbreak.
Strategy
The primary goal of the CDC during the 2009 H1N1 event was to “reduce transmission and illness severity, and provide information to help health care providers, public health officials and the public address the challenges posed by the new virus” (CDC, 2010c, p. 13). The response team’s primary strategy—rooted in emergency risk communication principles—was to develop a communication strategy that would provide accurate and timely information to the public regarding the H1N1 outbreak. Throughout the epidemic, the CDC sought to clearly communicate its goals and intended actions for responding to the situation. Communication strategists sought to harness the power of social media channels to complement traditional media strategies and thus allow the CDC maximum reach and impact with its “consistent, clear” message (CDC, 2010c, p. 13). The CDC based its messages around three core values: Be first, be right and be credible (CDC, 2010d). Message strategies included information regarding H1N1 preventative measures, symptoms, and treatment options.
The CDC relied on a strategic mix of traditional communication tools as well as the introduction of emergent technologies in its response to the H1N1 event. Traditional communication methods included maintaining a 24-hour national contact center (CDC-INFO), media relations, and health alert networks email, providing a variety of factsheets, flyers and brochures available for free download, and establishing a dedicated website for the H1N1 epidemic. The CDC also translated key materials and web pages into multiple languages, including a Spanish version of its 2009 H1N1 website. Newer methods included podcasts, the use of social networking sites (e.g., Facebook, Twitter), and the focus of this case study, YouTube (CDC, 2010d). It is especially significant to note that this integrated communication approach allowed the CDC to use its communication tools across multiple platforms. Links to videos and other informational resources could be posted on the Facebook pages as well as the CDC’s various Twitter accounts, enabling the CDC to reach a diverse audience across multiple social media sites.
Execution
As the number of H1N1 cases rapidly grew, the CDC sought to respond to the public’s need for information via a variety of mass communication formats. Although traditional public relations tools were an integral part of its strategy, the use of YouTube videos provided the CDC a relatively quick and highly accessible means to deliver information to the public (see Figure 1). As the outbreak quickly became a global issue, the use of YouTube videos also allowed for wide geographic distribution.
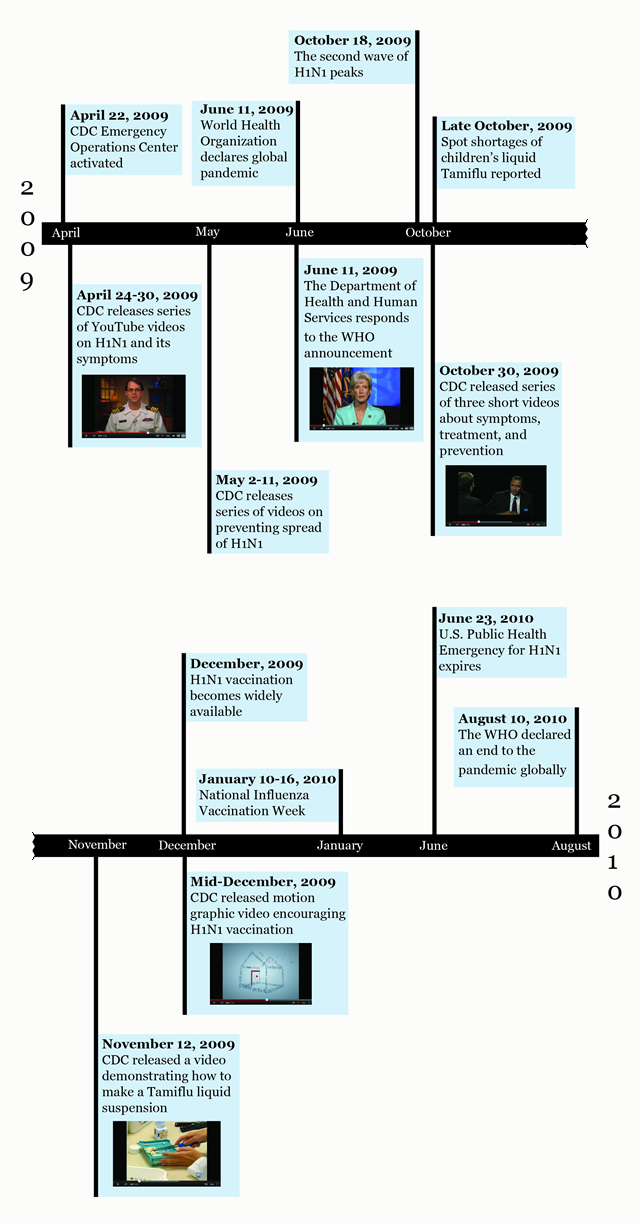 Figure 1. Timeline of YouTube videos posted by the CDC. Click a video cell to watch a YouTube video in a new window.
Figure 1. Timeline of YouTube videos posted by the CDC. Click a video cell to watch a YouTube video in a new window.
In its effort to quickly provide relevant and essential information regarding the spread and treatment of H1N1 flu, the CDC relied on simple and straight-forward production for its YouTube videos. Most of its early productions were shot from one angle with variations between close-up and extreme close-up views. As the viewing numbers for the videos reflect, this “no frills” production approach was an effective means of asynchronously presenting the necessary information. Millions of people were seeking accurate and reliable information about the H1N1 epidemic and the CDC placed the information on YouTube where the public would have 24-hour access. Names and titles of CDC officials were frequently used in the lower-third of the YouTube videos to identify key speakers and their official roles in addressing the H1N1 epidemic. This was an effective nonverbal communication strategy used to reinforce the CDC’s credibility and trustworthiness in the situation.
As the crisis progressed, the YouTube videos began to include slightly more variation in theme and content, with B-Roll footage under voice-overs being utilized as a regular production feature. In latter stages, cartoon characters were featured in the CDC’s productions with the launch of “The Happy Hand-washing Song” and high-quality motion graphics were featured in the 60-second “I never get the flu” YouTube production. These videos were a diversion from the CDC’s straight-forward approach to presenting relevant information to the public and, interestingly, only captured about 12,000 views combined. Due to the gravity of the situation and the likelihood that users were seeking straightforward facts about the H1N1 epidemic, it is likely these more “flashy” and graphically-focused pieces were not as effective in dissemination of the information sought. Alternately, the timing of these videos may have contributed to their low popularity, as the initial wave of H1N1 had passed.
Although the production quality and theme variation of the CDC’s YouTube videos increased during the public health crisis, the videos consistently sought to create a general sense of concern and urgency regarding protection and treatment of H1N1. Nearly all the videos covered the basics of protecting oneself from the virus: 1) Covering nose/mouth when coughing or sneezing; 2) Washing hands often; and 3) Avoiding contact with sick persons and staying home if diagnosed with H1N1. Several videos focused solely on providing this information to viewers. Information about H1N1 symptoms and when to seek treatment―including warning signs and steps to receive H1N1 care―were clearly stated and reinforced throughout the majority of the YouTube videos.
Evaluation
The World Health Organization (WHO) International Health Regulations (IHR) Emergency Committee officially declared the H1N1 influenza pandemic over on August 10, 2010 (CDC, 2010c). In the wake of the epidemic, the CDC sought to evaluate its efforts with a variety of measures, including web analytics, social media tracking, observation, and feedback from stakeholders. In a June 2010 “Summary Highlights” report, the CDC described its response to the H1N1 epidemic within the U.S. as a “complex, multi-faceted and long-term” reaction to a national health crisis (CDC, 2010b, p. 1).
This communication effort resulted in tremendous reach. The CDC estimates its risk communication campaign resulted in 403 million impressions from article placement in print and internet news media outlets alone (CDC, 2010b).[3] While the CDC does not report the estimated reach through other traditional media outlets, such as radio ads, television public service announcements, and printed materials, estimates of additional reach through nontraditional media are substantial. One report cited the CDC-INFO contact center had handled 212, 368 inquiries about the virus—141,774 general public phone calls, 47,311 general public emails, 23,268 clinician phone calls and 13 letters (CDC, 2010d). The CDC’s Facebook fan page grew by more than 55,000 individuals and one report cited more than 1.2 million followers of the CDC emergency profile on Twitter and nearly 34,000 followers of its @CDC_eHealth Twitter account (CDC, 2010d). In just the first three weeks of the response, the CDC website grew from one page to more than 200 with estimates of page views reaching 221 million (CDC, 2010d). Although one report mentions Facebook and Twitter analytics and website page views, it makes no mention of the fact that the 24 YouTube videos that compiled the CDC’s “2009 H1N1 playlist” reached well over 3 million views (CDC, 2010b).
Analysis and Discussion
This case study provides information essential to understanding the CDC’s response to the H1N1 epidemic. The CDC is considered a leader in the recent movement to combine the best practices of risk communication and crisis communication, and this case study provides significant support for its efforts to articulate that the response to global threats to the public must be “strategic, broad based, responsive and highly contingent” (Reynolds & Seeger, 2005, p. 49). Reynolds and Seeger (2005) argue the crisis and emergency risk communication (CERC) model is a “blended form of communication” that “emphasizes the developmental features of crisis and the various communication needs and exigencies of audiences at various points in the ongoing development of an event” (p. 49). The CERC model posits that crises generally have five distinct stages: 1) Precrisis, 2) Initial event, 3) Maintenance, 4) Resolution, and 5) Evaluation.[4]
While the CDC continued to rely on traditional and more conventional communication tactics such as media relations, web sites, and printed materials, this study illustrates the necessity of making vital public health messages accessible to the general public on YouTube. At more than 3 million views, the number of views for the CDC-produced H1N1 videos broadcast on YouTube indicates that a significant number of individuals were interested in information relevant to the 2009 H1N1 epidemic. Additionally, it emphasizes the importance of public health entities being willing to adapt to the changing nature of information dissemination in the face of innovative technologies and new media.
The CDC remains a highly credible source for public health information, and has recognized and responded to the need to expand its strategic communication boundaries to include new media by launching accounts in a variety of social media domains and developing best practices for the use of social media for public health communication (see the CDC Social Media Toolkit for Health Communicators). Their guidelines for the use of YouTube suggest that health communicators develop content appropriate for target audiences, keep videos short, and maximize production quality—all qualities found in the videos produced for the response to 2009 H1N1 flu. In the case presented here, the CDC was able to use a relatively new technology, YouTube, to deliver a consistent public health message to a widely varied mass audience during a national health crisis.
Discussion Questions and Activities
- Although YouTube is an extremely popular social media site, it often features material that is poorly sourced or may lack credibility (e.g., may not be considered “official” or trustworthy by the viewer). What risks was the CDC taking by using YouTube as a communication channel during a national public health crisis? Do you think the benefits of using YouTube outweighed the risks in this situation? Why or why not?
- The use of YouTube during a national health crisis gives rise to many questions about the changing nature of strategic communication, specifically during health-related crises. Is the lessening dependence on traditional news media as a mass communication vehicle a positive or a negative shift? Explain your position.
- Small group exercise: Given what you know about the CDC’s use of YouTube during the H1N1 epidemic, how would you build on it to create a comprehensive social media strategy for responding to this national public health crisis? Decide which social media tools or channels you would select and what kinds of messages you would use in each channel.
- In addition to its YouTube campaign, the CDC relied on other popular social media platforms, such as Facebook and Twitter, to distribute its health-focused message. How has the proliferation of social media changed the way we seek and use health-related information? What impact has this had on health professions and the practice of health communication?
Notes
[1] Initial reports linked the H1N1 virus to a swine origin influenza virus because the combination of genes closely resembled those of the North American and Eurasian swine-lineage H1N1 influenza viruses. From December 2005 to January 2009, 11 of the 12 cases of human infection reported either direct exposure or close proximity to pigs. The April 2009 cases in the U.S., however, did not involve exposure to pigs, thus the new virus was being spread via human to human contact and not human-to-swine. When the CDC confirmed there was no link between the spread of the H1N1 virus and pigs, an effort was made to identify the virus as “2009 H1N1” (CDC, 2010b, p. 1-2).
[2] The 2009 H1N1 outbreak was a complex event that required a coordinated response from multiple countries, the World Health Organization, the Pan American Health Organization, and the global public health community (Brownstein, Freifeld, & Madoff, 2009). While this case study focuses specifically on the response of the Centers for Disease Control and Prevention in the U.S. in an attempt to provide a vivid example of how an organization can use social media to meet strategic communication goals, it is important to note that this case was situated within a global response effort. The use of YouTube allowed CDC to meet its domestic communication goals, and these videos were publicly, and thus globally, available for those with open access to the internet.
[3] Media monitoring at CDC takes many forms, including traditional clipping services, automated programs (Janssen, Haag, & Pierre, 2010), and systems that involve manual searching and coding by trained staff members. During an emergency activation, media monitoring activities are concentrated in the Joint Information Center and result in periodic summary reports that are used to provide situation updates to leadership, inform communication strategy, and track communication efforts (see Prue, Lackey, Swenarski, & Gantt, 2003, for an example).
[4] Within the five stages of the CERC model, communication strategies for the organization vary based on the characteristics of the given crisis. Generally, they are as follows: 1) Precrisis: risk messages, warnings, and preparations; 2) Initial event: uncertainty reduction, self-efficacy, reassurance; 3) Maintenance: ongoing uncertainty reduction, self-efficacy, reassurance; 4) Resolution: updates regarding resolution, discussions about cause and new risks/understanding of risk; and 5) Evaluation: discussion of adequacy of response, consensus about lessons and new understandings of risks (Reynolds & Seeger, 2005, p. 52-53).
References
American Red Cross. (2010). Social Media in Disasters and Emergencies. Retrieved from http://www.redcross.org/www-files/Documents/pdf/other/SocialMediaSlideDeck.pdf
Brownstein, J. S., Freifeld, C. C., & Madoff, L. C. (2009). Influenza A (H1N1) Virus, 2009—Online monitoring. The New England Journal of Medicine, 360, 2156.
Centers for Disease Control and Prevention (2010a). CDC Fact Sheet. Retrieved from http://www.cdc.gov/about/resources/facts.htm
Centers for Disease Control and Prevention (2010b). The 2009 H1N1 pandemic: Summary highlights, April 2009-April 2010. Retrieved from http://www.cdc.gov/h1n1flu/cdcresponse.htm
Centers for Disease Control and Prevention (2010c). 2009 H1N1 Flu. Retrieved from http://www.cdc.gov/h1n1flu/
Centers for Disease Control and Prevention (2010d). 2009 H1N1: Overview of a Pandemic. Retrieved from http://www.cdc.gov/h1n1flu/yearinreview/yir8.htm
comScore, Inc. (2009). YouTube surpasses 100 million U.S. viewers for the first time: Americans’ time spent viewing jumps 15 percent versus previous month. Retrieved from http://www.comscore.com/Press_Events/Press_Releases/2009/3/YouTube_Surpasses_100_Million_US_Viewers
Ignite Social Media, Inc. (2012). 2011 Social Network Analysis Report – Geographic – Demographic and Traffic Data Revealed. Retrieved from http://www.ignitesocialmedia.com/social-media-stats/2011-social-network-analysis-report/
Janssen, A., Haag, E. S., & Pierre, J. (2010, April). Rapid and longitudinal analysis of H1N1 News and Social Media. Paper presented at the 44th National Immunization Conference, Atlanta, GA. Abstract retrieved from http://cdc.confex.com/cdc/nic2010/webprogram/Paper22799.html
Janssen, A. P., Tardif, R. R., Landry, S. R., & Warner, J. E. (2006). “Why tell me now?” The public and healthcare providers weigh in on pandemic influenza. Journal of Public Health Management and Practice, 12, 388-394.
Prue, C. E., Lackey, C., Swenarski, L., & Gantt, J. M. (2003). Communication monitoring: Shaping CDC’s emergency risk communication efforts. Journal of Health Communication, 8, 35–49.
Reynolds, B. (2007). Crisis and Emergency Risk Communication: Pandemic Influenza. Washington, DC: Government Printing Office.
Reynolds, B. J. (2010). Building trust through social media. CDC’s experience during the H1N1 influenza response. Marketing Health Services, 30, 18-21.
Reynolds, B., & Seeger, M. W. (2005). Crisis and emergency risk communication as an integrative model. Journal of Health Communication, 10, p. 43-55.
Zuckerberg, M. (2009, April 8). 200 million strong [Weblog post]. Retrieved from http://blog.facebook.com/blog.php?post=72353897130
LAURA RICHARDSON WALTON, Ph.D., APR, is an assistant professor in the Department of Communication at Mississippi State University. She is also a Research Fellow and Coordinator of the Media Collaboration Laboratory in the Social Science Research Center. Email: lwalton[at]comm.msstate.edu.
HOLLI H. SEITZ, MPH, is a doctoral student studying health communication in the Annenberg School for Communication at the University of Pennsylvania.
KATHLEEN RAGSDALE, Ph.D., is an assistant research professor at the Mississippi State University Social Science Research Center. She is an applied medical anthropologist who is currently conducting mixed method research on how new media/electronic technologies can be harnessed to address health disparities among minority and vulnerable populations, with a particular focus on high risk behavior prevention among rural and at-risk youth.
The preparation of this manuscript was supported by the Social Science Research Center (SSRC) at Mississippi State University and the Annenberg School for Communication at the University of Pennsylvania. The authors gratefully acknowledge the contribution of research assistants Cameron White and Sydney Hall in the SSRC’s Media Collaboration Laboratory.
Editorial history
Received January 23, 2012
Revised April 9, 2012
Accepted April 18, 2012
Published May 13, 2012
Handled by editor; no conflicts of interest