

To cite this article
Ragsdale, K., Harper, S. K., Kathuria, S., Bardwell, J. H., Penick, C. B., & Breazeale, M. (2015). Social media to enhance sexual health education for youth: FactNotFiction’s (re)design and launch. Case Studies in Strategic Communication, 4, article 5. Available online: http://cssc.uscannenberg.org/cases/v4/v4art5
Access the PDF version of this article
Social Media to Enhance Sexual Health Education for Youth: FactNotFiction’s (Re)Design and Launch
Kathleen Ragsdale
Mississippi State University
Sydney K. Harper
Southern Alabama Area Health Education Center
Sheeji Kathuria
Mississippi State University
Jamie H. Bardwell
Women’s Foundation of Mississippi
Carol B. Penick
Women’s Foundation of Mississippi
Michael Breazeale
Mississippi State University
Abstract
Inadequate access to comprehensive sex education has been linked to adolescent childbearing in the U.S., which has the highest teen birth rate among comparable developed nations as well as disproportionately high rates of sexually transmitted infections (STIs) among youth and young adults. Resource-limited states such as Mississippi experience high rates of adolescent childbearing and STIs. For example, at 42.6 births per 1,000 teen girls, Mississippi has the third highest adolescent birth rate in the nation. Although 58% of Mississippi high school students are sexually active, the delivery of comprehensive sex education in public schools faces a number of issues in Mississippi (e.g., a ban on condom use demonstrations). In order to fill the critical gap in comprehensive sex education in Mississippi public schools, FactNotFiction was launched in 2012 to provide medically-accurate sexual and reproductive health information (i.e., comprehensive sex education) to Mississippi teens. We describe challenges associated with FactNotFiction’s initial development and launch and its successful redesign. Lessons learned from addressing FactNotFiction’s challenges have implications for other eHealth and social media initiatives for public health promotion—especially those targeting youth.
Keywords: comprehensive sex education; abstinence-only education; teen pregnancy prevention; eHealth; social media
Introduction
At 31.3 births per 1,000 girls ages 15 to 19, the United States (U.S.) has the highest teen birth rate among comparable developed countries such as the United Kingdom (21.8), Australia (15.9), Canada (14.1), and the Netherlands (4.8) (NCPTUP, 2015a). The U.S. also has disproportionately high rates of sexually transmitted infections (STIs) among youth/young adults ages 15 to 24 (CDC, 2015a). Resource-limited states such as Arkansas, Louisiana, and Mississippi report especially high rates of teen childbearing and STIs among youth/young adults—particularly among African Americans (Boonstra, 2014; CDC, 2015a; Ragsdale & Sutton, 2012). For example, Mississippi ranks third in rate of births among girls ages 15 to 19 (CDC, 2015a; NCPTUP, 2015b), with African American teen girls most impacted (54.7 births per 1,000 as compared to 38.9 births per 1,000 among non-Hispanic whites) (NCPTUP, 2015b). Mississippi also ranks third in rate of gonorrhea and fifth in rate of chlamydia among youth/young adults ages 15 to 24 (CDC, 2015a).
Comprehensive sex education—also referred to as abstinence-plus education—teaches youth that abstinence is the best way to prevent unintended pregnancy and STIs while also providing youth with 1) age-appropriate and medically accurate information on condoms and contraceptives and 2) interpersonal and communication skills to help “young people explore their own values, goals, and options” (Advocates for Youth, 2015a, p. 1) and make responsible decisions around dating, relationships, and sexual activities (SIECUS, 2009). Research suggests that inadequate access to comprehensive sex education is associated with increased risk for STIs and adolescent childbearing in the U.S. (Goldman, 2011; Kohler et al., 2008; Stanger-Hall & Hall, 2011). Yet implementing comprehensive sex education in U.S. public schools is highly politicized (Santelli, Ott, Lyon, Rogers, Summers, & Schleifer, 2006; Santelli & Kirby, 2010; Stanger-Hall & Hall, 2011; Tortolero, Johnson, Peskin, Cuccaro, & Markham, 2011). Although comprehensive sex education detractors often cite parental support for abstinence-only education as a key factor behind legislative efforts to mandate abstinence-only education in U.S. public schools, a number of studies suggest parents are supportive of comprehensive sex education for their children. For example, results of a 2010 survey conducted in Texas—considered a politically conservative state—among 1,201 parents of school-aged children were aligned with “peer-reviewed published national and statewide surveys of parents and the general public” in their strong support for comprehensive sex education (Tortolero et al., 2011, p. 2). Likewise, results of a 2011 survey conducted in Mississippi—also considered a politically conservative state—among 3,600 parents of school-aged children also indicate strong support for comprehensive sex education (McKee, Ragsdale, & Southward, 2014). For example, 92% of parents in the Mississippi sample support age-appropriate sex education in public school, 82% support teaching basic information related to reproduction and pregnancy, and 61% support implementation of sex education in middle school (i.e., grades 5 to 7) (McKee, Ragsdale, & Southward, 2014).
Prior to the passage of House Bill 999 (HB 999) by the State Legislature in 2011, Mississippi public school districts were not required to provide sex education. A key component of HB 999 mandates that every local public school board in the state must implement abstinence-only or abstinence-plus education into the curriculums of its public schools during the 2012-2013 academic year (Mississippi State Legislature, 2011). HB 999 also mandates that “abstinence-only education shall remain the state standard for any sex-related education taught in the public schools” (Mississippi State Legislature, 2011, p. 2). The bill includes six key components that define abstinence-only education, including that “a mutually faithful, monogamous relationship in the context of marriage is the only appropriate setting for sexual intercourse” (Mississippi State Legislature, 2011, p. 3, emphasis added). Interestingly, abstinence-only education is not required to include all six components (although it must not contradict them), while abstinence-plus education must include all six components (Mississippi State Legislature, 2011; SIECUS, 2014). As of June 2012 (the deadline set forth by HB 999), 53% of Mississippi’s 152 public school districts (N=81) adopted abstinence-only education and another three public school districts adopted an abstinence-only education for younger grades and abstinence-plus education for older grades (Pettus & Amy, 2012).
The delivery of comprehensive sex education in Mississippi public schools faces a number of issues due to constraints embedded within HB 999. First, Mississippi is one of only three states that require parents to provide consent before their children can attend sex education classes (Kempner, 2014; NCSL, 2015). This mandatory parental “opt-in” policy within HB 999 not only creates an additional burden for parents, but may also contribute to creation of an “overtly moralistic” environment not conducive to the delivery of school-based sex education (Miedema, Maxwell, & Aggleton, 2011, p. 516). Researchers argue that overtly moralistic environments can constrain educators in their delivery of comprehensive sex education due to real or perceived concerns regarding “push-back” from school administrators and other stakeholders (Brewin, Koren, Morgan, Shipley, & Hardy, 2014; Eisenberg, Madsen, Oliphant, & Sieving, 2013; Miedema, Maxwell, & Aggleton, 2011). Second, HB 999 requires that school-based sex education is taught in same-sex groups, which may not only reinforce sexism and gender stereotyping but may create an additional implementation burden among Mississippi public schools that are already resource-limited (Goodkind, Schelbe, Joseph, Beers, & Pinsky, 2013; Halpern et al., 2011).
Third, as is the case in a number of U.S. states (NCSL, 2015), HB 999 does not mandate that sex education is required to provide medically accurate information. A cornerstone of comprehensive sex education is providing youth with “complete, accurate, and age-appropriate sex education that helps them reduce their risk of HIV/AIDS, other sexually transmitted infections (STIs), and unintended pregnancy” (SEICUS, 2009, p. 1). In contrast, abstinence-only education has been found to be “ineffective…in promoting pubertal wellbeing, risk protection and reproductive health [as] compared with comprehensive, multi-focal and evidence-based programs” (Goldman, 2011, p. 527; see also Advocates For Youth, 2015a; SEICUS, 2009).
Fourth, HB 999 prohibits condom use demonstrations during school-based sex education, regardless of whether the curriculum is abstinence-only or abstinence-plus. Restrictions on specific curriculum content have been identified as a challenge to comprehensive sex education in other states and can be especially detrimental to youth who are currently sexually active (Kelsey & Layzer, 2014; Ott et al., 2011; Ragsdale & Sutton, 2012). Such issues related to the constraints embedded within HB 999 suggest important gaps in access to comprehensive sex education among Mississippi youth.
These gaps are of particular concern given that—as compared to high school students nationwide—Mississippi high school students are more likely to, for example, currently be sexually active and have had four or more sex partners (CDC, 2015b). In fact, data from the 2011 Mississippi Youth Risk Behavior Survey indicate that—among Mississippi students who are sexually active—63% of boys are sexually active by age 13 and 65% of girls are sexually active by age 16 (Ragsdale & Sutton, 2012). In addition to Mississippi’s high teen birth rate mentioned previously, it is important to note that 20% of these adolescent births are repeat births (U.S. Departement of Health and Human Services, 2014).
In order to meet the need to increase access to medically accurate sexual and reproductive health information among Mississippi youth, the Women’s Foundation of Mississippi launched the FactNotFiction website in 2012 to provide evidence-based sexual and reproductive health information specifically tailored to appeal to youth. In this paper, we present a case study of two major challenges associated with the development and design of the FactNotFiction website and how we addressed these challenges.
Background: FactNotFiction’s Development
Initially launched on October 1, 2012, the purpose of the FactNotFiction website is to provide medically accurate sexual and reproductive health information to teens—and their parents—on topics such as teen pregnancy prevention, HIV/STI prevention, correct condom use, contraceptives, healthy dating relationships, and parent/teen communication about sexual and reproductive health. The organizations initially involved in the FactNotFiction project included the Women’s Foundation of Mississippi, Youth+Tech+Health (YTH, formerly ISIS Inc.), and The Ramey Agency, each of which had a different role in the project. The FactNotFiction project was initiated and directed by the Women’s Foundation of Mississippi, a grant funding and advocacy organization dedicated to advancing programs that improve the lives of women and girls statewide.
The content for the FactNotFiction website and development of the initial website design was led by the California-based YTH, which includes a team of public health professionals who create content for sexual health education websites targeting youth. FactNotFiction’s statewide media campaign to build awareness of the website among Mississippi youth and parents was led by the Mississippi–based Ramey Agency and conducted over a two-year period. The media campaign included developing and executing an integrated launch/brand campaign of the FactNotFiction website via traditional media channels (e.g., television, radio, transit ads) and social media channels (e.g., Facebook, Twitter).
The FactNotFiction website and media campaign were designed with input from a Youth Advisory Council convened by the Women’s Foundation that included ten youth/young adults ages 15-20 years. Human subjects protection of members of the Youth Advisory Council was approved by the Women’s Foundation and Council members received a $100 stipend for their service and a $25 stipend to cover their transportation costs. In addition to one in-person meeting of all members of the Youth Advisory Council, members regularly communicated via a private Facebook page created for this purpose. Council members’ primary responsibilities included providing feedback on FactNotFiction’s design and content and feedback on the media campaign materials used to promote the website.
Challenge 1: Structure and Design
The FactNotFiction website was created to provide medically accurate sexual and reproductive health information to teens and parents in an accessible and appealing format. Based on research that 91% of Mississippi households with children under age 18 have access to the Internet (Beaulieu & Gallardo, 2012) and 78% of youth ages 12 to17 have mobile phones (of which 47% are smartphones) (Madden, Lenhart, Duggan, Cortesi, & Gasser, 2013), we anticipated a strong mobile audience for the FactNotFiction website. However, based on their prior experience with minority youth in California, the YTH web developer did not create a mobile-enabled version of the FactNotFiction website. The rationale behind the YTH web developer’s decision to forego a mobile-enabled site for FactNotFiction was based on YTH research that low income teenagers have mobile phones with Internet capabilities, but that these mobile phones are not necessarily smartphones.
On December 13, 2012, we reviewed data from Google Analytics to evaluate the success of the first 43 days of FactNotFiction (October 3–December 13, 2012) as measured by five key performance indicators (KPIs) including 1) percentage of mobile device visitors, 2) number of visitors per day, 3) geographic distribution of visitors, 4) duration of each site visit, and 5) bounce rate. Google Analytics is a free Google service that generates detailed statistics about a website’s visitors (Google Analytics, 2015a). While Google Analytics has received some criticism for being difficult to use and for potentially underestimating the time visitors actually spend on a site, it is still considered the industry standard for website statistics tracking (Melaugh, 2014).
We were not surprised that the KPI metrics indicated that mobile devices accounted for 71% of visits to the FactNotFiction website. However, contrary to expectations of YTH, the KPI metrics indicated that the top three devices used to visit FactNotFiction included two smartphones—the Apple iPhone (N=3,600 visits) and Samsung SCH-I500 Fascinate (N=873 visits)—as well as the Apple iPod (N=923 visits). The KPI metrics also indicated that there were 8,848 visits to the FactNotFiction website during its first 43 days post-launch. The developers’ and researchers’ own web addresses were excluded from the analysis so as not to artificially inflate the number of site visits.
Eighty-eight percent of visitors to the FactNotFiction website during this time frame (October 3–December 13, 2012) were first-time visitors to the website (i.e., “new visitors”), which highlights the problematic fact that only 12% of site visitors were returning to the FactNotFiction website at a later date. Sixty-four percent of visitors to the FactNotFiction website during this time frame were Mississippi residents. Visitors stayed on the FactNotFiction website for an average 0.47 minutes and visited an average of 1.5 pages. When taken as a whole, the KPI metrics clearly indicate that our target audience was not highly engaged with the FactNotFiction website during the first 43 days after it launched.
The most straight-forward KPI metric that the FactNotFiction website was not meeting expectations was the bounce rate, which is the percentage of visitors who visit only one web page (usually the landing page) before exiting a site (Google Analytics, 2015b). The bounce rate of 54% among desktop users visiting the original FactNotFiction website was within the Google Analytics “acceptable” range of 40-60% (Kelly, 2015). In contrast, the bounce rate of 79% among mobile phone users visiting the original FactNotFiction website was unacceptably high. Based on the KPI metrics that indicated that 1) a high number of smartphone users were visiting the site, 2) the average number of pages visited was 1.5, and 3) there was a high bounce rate among mobile phone users visiting the site, we re-evaluated the YTH web developer’s assumption that Mississippi youth have mobile phones but not necessarily smartphones, which was a key assumption that had initially guided FactNotFiction’s website design.
Challenge 2: Content and Delivery
FactNotFiction is a relatively static website in that it has fixed content rather than dynamic content generated in real-time. The website’s 31 topic tabs include, for example 1) sex, 2) pregnancy, 3) condoms, 4) abstinence, 5) HPV, 6) Ask the Expert!, and 7) Find A Health Center Near You. The only FactNotFiction website content that changes regularly is under the Ask the Expert! tab, where youth submit anonymous questions to a team of health care professionals who provide answers that are posted on the site. Google Analytics indicated that, although traffic remained steady from the website’s initial launch on October 1, 2012, through the end of that year, there was a significant drop in traffic once the promotional campaign ended on December 31, 2012. For example, the FactNotFiction website had 15,783 visitors from October 1 to December 31, 2012, as compared to 3,466 visitors from January 1 to April 4, 2013.
In addition to its website, FactNotFiction has a Facebook page with the goal to push traffic to the website. In contrast to the relatively static website, the FactNotFiction Facebook page is dynamic because it has a dedicated staff person at The Ramey Agency who produces daily content for the Facebook page. We used Facebook Insights to analyze the effectiveness of the FactNotFiction Facebook page. Facebook Insights allows site owners to track the number of likes a page or individual posts receive. It also tracks the number of reposts, which is an indicator of the reach and engagement generated by page content. Although Facebook Insights is superior to Google Analytics in terms of simplicity of use, it lacks the ability to track subsequent reposts after content has been posted to other sites (Allard, 2013). Data from Facebook Insights indicated that the FactNotFiction Facebook page had 11,635 likes from March 30 to April 26, 2013 (see Table 1). Of these Facebook likes, 59% were from youth ages 13 to 17 and 37% were from young adults ages 18 to 24. In addition, the top 20 cities from which these Facebook likes were generated are all within Mississippi.
Table 1. Facebook Insights statistics of site visitors by gender and age from March 30 to April 26, 2013.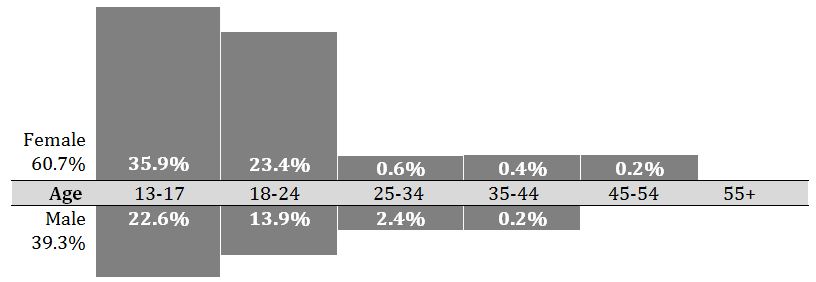
Based on our review of the Google Analytics and Facebook Insight metrics, we concluded that project’s primary target audience of Mississippi youth and young adults are more engaged with FactNotFiction’s dynamic Facebook page than with the static website. Indeed, Google Analytics’ engagement statistics suggest that the FactNotFiction website was functioning more as a reference page where visitors went when they had particular sexual health or reproductive questions or concerns (e.g., where to find a local health clinic). In contrast, Facebook Insights’ engagement statistics—which track “high traffic” indicators such as likes, shares, and comments—suggest that the FactNotFiction Facebook page had evolved into an interactive social environment for youth. We believe this was due to our strategy to develop and post content on the FactNotFiction Facebook page that is purposively formatted to be dynamic and, therefore, more appealing and accessible to youth. Based on the higher number of visitors to the FactNotFiction Facebook page as compared to the FactNotFiction website, we re-evaluated the YTH web developer’s assumption that youth will return to a sexual and reproductive health website even if it is static—another key assumption that had guided FactNotFiction’s initial website design.
Addressing FactNotFiction’s Challenges
After reviewing data from Google Analytics and Facebook Insights for the first several months after FactNotFiction’s launch, we decided to make several changes to FactNotFiction’s structure, design, and content. For example, instead of having one organization manage the FactNotFiction website and another organization manage the FactNotFiction promotional campaign, we transferred both responsibilities to The Ramey Agency, as the logistics of working with a non-local organization became more challenging and time-consuming as the FactNotFiction project moved forward. The Ramey Agency recommended two overlapping changes to FactNotFiction to address the challenges previously discussed. These recommendations and their outcomes are detailed below.
Recommendation and Outcome to Address Challenge 1
The Ramey Agency recommended that we increase website traffic and reduce the bounce rate by making the FactNotFiction website mobile-enabled for smartphones and by presenting the site in a format more similar to what youth were already using, such as Tumblr. A microblogging platform and social networking site, Tumblr allows users to post text, audio, video, and images to a site using a browser, mobile phone, desktop, or email account. Tumblr users are known to be both young and “incredibly engaged” with using the site (Smith, 2013). As Smith (2013) explains,
unlike networks that encourage quick messaging and brief glances at the feed, Tumblr’s emphasis on multimedia blog posts means users spend a fair amount of time creating and digesting what’s on the site. More total time is spent on Tumblr than on bigger social networks like Twitter, LinkedIn, and Pinterest. (p. 1)
Although, as mentioned previously, there was initial concern that FactNotFiction’s primary target audience of Mississippi youth would not have smartphones, Google Analytics’ engagement statistics indicated that 79% of visitors accessed the FactNotFiction website via a smartphone. Therefore, the original FactNotFiction website was converted into a Tumblr site on April 5, 2013. It is important to note that—because all content lives on a single scrollable Tumblr site—we anticipated that the FactNotFiction Tumblr site’s bounce rate would remain high due to how bounce rate is calculated. Therefore, the primary KPI for the FactNotFiction Tumblr site is time spent on the site (i.e., site visit duration).
Google Analytics indicated the average visit duration on the FactNotFiction Tumblr site increased to 2.32 minutes from April 6 to April 29, 2013, as compared to an average of 0.47 minutes from October 3 to December 13, 2012, on the original FactNotFiction website. This is nearly a five-fold increase in visitor engagement during the 24 days after converting FactNotFiction from a static website into a Tumblr site. This dramatic increase in average visit duration illustrates the success of our Tumblr site conversion strategy. Additionally, The Ramey Agency used behavior targeting through online and mobile media to select specific websites based on web-browsing behaviors among youth in order to drive traffic to the FactNotFiction website.
Behavior targeting is an advertising mechanism used to gain a better understanding of particular populations by collecting information on their web-browsing behaviors (BFM, 2013). This information allows an organization to strategically place advertisements on websites frequented by the targeted audience in order to drive traffic to the organization’s website. Due to the fact that Mississippi youth who are African American are most at-risk for STIs and adolescent childbearing (CDC, 2015a; NCPTUP, 2015b; Ragsdale & Sutton, 2012), The Ramey Agency strategically selected specific websites popular among African American youth on which to advertise FactNotFiction in order to optimize outreach to this particular demographic.
Recommendation and Outcome to Address Challenge 2
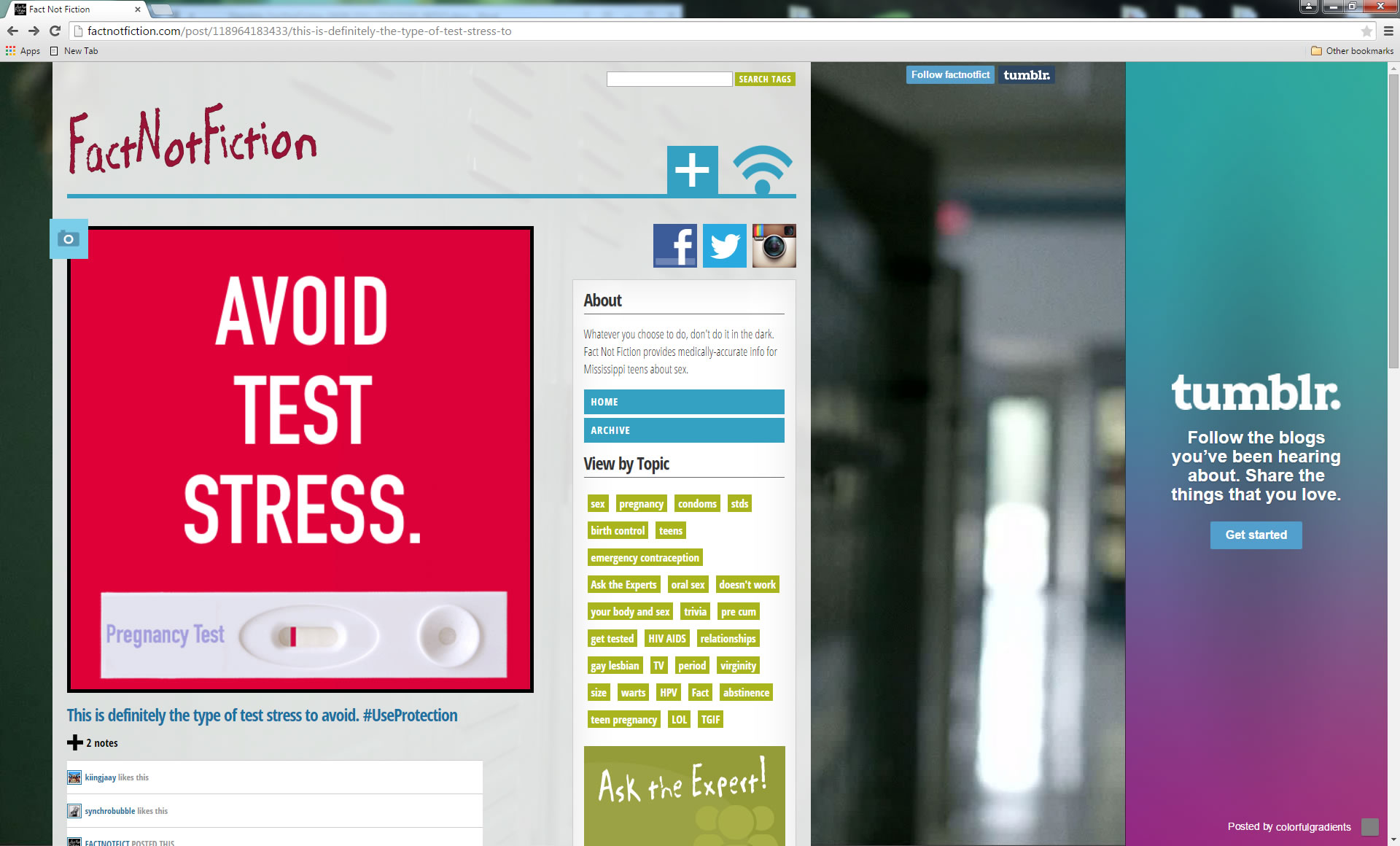
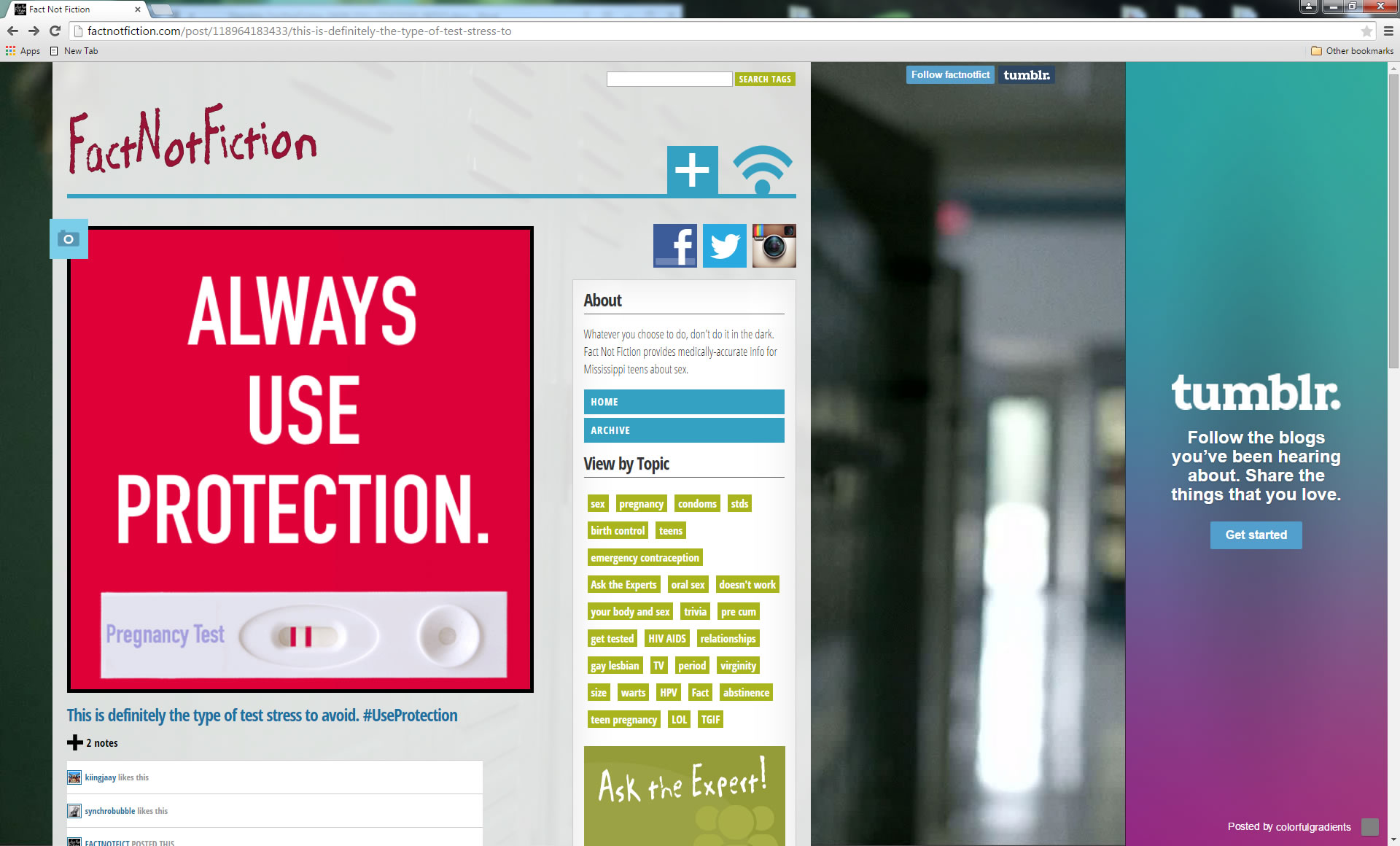
As mentioned above, The Ramey Agency recommended that we increase website engagement by converting FactNotFiction’s static website into a Tumblr site in order to create a more dynamic experience for visitors. By allowing visitors to post text, audio, video, and images, the FactNotFiction Tumblr site blends the positive aspects of the original website (e.g., medically accurate and easy-to-access sexual and reproductive health information) with the dynamic interface of the FactNotFiction Facebook page to create an interactive, visual experience for Mississippi youth. See Figures 1 and 2 for examples of content under the ‘sex’ tab on the FactNotFiction’s Tumblr site.
In order to maintain continuity, the FactNotFiction Tumblr site has the same address as the original website—www.factnotfiction.com—and contains a link to the original version of the full website (http://factnotfictionms.com/) (see Figure 3). The goal of the FactNotFiction Tumblr site is to convert Facebook page visitors to website visitors. Therefore, all content posted to the FactNotFiction Facebook page is also posted to the FactNotFiction Tumblr site so that the site is constantly updated. The Google Analytics used to track the FactNotFiction Tumblr site’s success since its launch on April 5, 2013, indicate that the number of visitors to the FactNotFiction site has increased, as has the average visit duration.

Analysis and Discussion
The CDC has effectively used social media to track flu, disease, and foodborne illness outbreaks across the nation and to predict where outbreaks are imminent in a practice they call “nowcasting” (Nsoesie, 2014). But can social media be used more proactively to disseminate public health information? Although the literature is still emerging, evaluations to determine whether the strategic use of social media is an effective way to deliver targeted public health education suggest it is promising. For example, the CDC successfully addressed the 2009 H1N1 flu epidemic by developing a public health response plan that included the dissemination of targeted content on social media platforms where the CDC had not yet established a presence, including Facebook and YouTube (Walton, Seitz, & Ragsdale, 2012). Likewise, an evaluation of the AfterTheInjury.org intervention for parents of injured children found that parents who received the intervention via an interactive website were significantly more likely to indicate that they would access the web content in the future as compared to parents who received the intervention as a stand-alone DVD (Marsac, Kassam-Adams, Hildenbrand, Kohser, & Winston, 2011).
Although this literature is also still emerging, evaluations to determine whether the strategic use of social media is an effective way to deliver sexual health and prevention information to youth who may be at heightened HIV/STI risk—such as sexually active youth and young men who have sex with men (YMSM)—is also promising (Bull, Levine, Black, Schmiege, & Santelli, 2012; Carpenter, Stoner, Mikko, Dhanak, & Parsons, 2010; Mak, Bastian, Grace, Aquilina, & Sweeting, 2012; McCarthy, Carswell, Murray, Free, Stevenson, & Bailey, 2012). Indeed, using mobile-enabled social media to deliver sexual health and HIV/STI prevention information may be extremely effective for at-risk youth, given the immense popularity of and reliance on mobile phones and the Internet among this hard to reach demographic (Madden, Lenhart, Duggan, Cortesi, & Gasser, 2013; Jones & Biddlecom, 2011; Smith, 2013). Another important advantage of using social media for distributing sexually sensitive health communications to at-risk youth is that it offers anonymity, interactivity, dynamic content, and a forum in which to convey age-appropriate and culturally tailored sexual health and risk-reduction information to this audience (Mak, Bastian, Grace, Aquilina, & Sweeting, 2012).
Although innovative efforts to harness social media to optimize sexual and reproductive health outreach to large numbers of youth are vitally needed, considerable knowledge gaps remain on how to design and launch effective youth-oriented sexual health and risk-reduction sites. Literature reviews by Dunne and colleagues (2014), Jones and colleagues (2014), and Simon and Daneback (2013) indicate that using social media to meet youth’s sexual health and risk-reduction needs is promising, as social media options may be feasible and cost-effective tools “to use for educating adolescents to make more informed sexual decisions” (Dunne, McIntosh, & Mallory, 2014, p. 401).
In this paper, we seek to add to this growing body of knowledge by presenting lessons learned from a case study of the (re)design and launch of FactNotFiction, a comprehensive sex education site specifically tailored to provide Mississippi youth with medically accurate sexual and reproductive health information. A limitation of this case study is that due to budget constraints we have had to rely on web-based analytic tools (e.g., Google Analytics, Facebook Insights) to inform the decision-making processes related to FactNotFiction’s design and content development. Although constructive, such analytic tools cannot (yet) fully answer such important questions as, “why did someone come to our site, what they want to accomplish [by visiting the site], what their emotional experience was like, what their eyes actually looked at, and what they told others later” about the site (Owyang, 2007, p. 1).
As Bull and colleagues (2012) note, a common limitation of emerging efforts to optimize comprehensive sex education for youth delivered via social media is that researchers have an “incomplete understanding of motivations for engagement with content on social media” (Bull, Levine, Black, Schmiege, & Santelli, 2012, p. 473). Continued research on why and how youth engage with online sexual and reproductive health content is urgently needed, as is research to improve eHealth literacy among youth, which is defined as “the abilities to find, evaluate, and apply online health information” (Paek & Hove, 2012, p. 727). For example, in an exploratory study of how youth use the Internet to access sexual and reproductive health information, researchers found that youth who use the Internet “proactively to educate themselves about contraception and safe sex were the exceptions rather than the rule” (Jones & Biddlecom, 2011, p. 116, emphasis added). Likewise, many youth express mistrust of online sexual health and risk-reduction resources or are unsure how to effectively evaluate whether such resources are trustworthy (Ghaddar, Valerio, & Garcia, 2012; Jones & Biddlecom, 2011). Such findings are reflective of the need to improve eHealth literacy among youth, especially those at heightened risk for unintended pregnancy and/or STIs.
In terms of the present eHealth project, several factors likely contributed to the improved reach and effectiveness of the FactNotFiction social media campaign. First, the shift from traditional media channels to disseminate promotional information about the FactNotFiction website (e.g., television, radio, transit) to behavioral targeting likely had a strong positive impact on improved outreach to the project’s primary target audience of Mississippi youth/young adults, and especially African Americans in this age group. By employing behavioral targeting of their promotional message, The Ramey Agency ensured that each person who saw the message was actually a potential member of FactNotFiction’s primary target audience.
Second, smartphone penetration was in an extreme growth phase during the time that the FactNotFiction social media campaign was being rolled out. While only a few months separated the original FactNotFiction website launch and the launch of the FactNotFiction Tumblr site, smartphone penetration in the U.S. rose from 50% to 57%, with a disproportionate amount of that growth attributed to the youth market (Statista, 2015). Interestingly, smartphone penetration tends to ignore many of the income and other demographic boundaries that have often define technology adoption, with adoption rates being fairly consistent across the general population (Anderson, 2015). Indeed, at FactNotFiction’s inception in 2012, YTH’s experience was that few minority teens had smartphones. But a survey administered in 2014-2015 to a nationally representative sample of 1,060 youth ages 13 to 17 by researchers with the Pew Research Center found that “African-American teens are the most likely of any racial or ethnic group to have or have access to a smartphone” (Lenhart, 2015, p. 8). Indeed, Lenhart (2015) found that “85% of African-American teens report smartphone ownership, compared with 71% of white and 71% of Hispanic youth” (p. 8).
Third, the use of the Tumblr platform improved not only the potential reach of the message but also the likelihood that FactNotFiction’s target audience would spend more time on the site once they discovered it. In terms of reach, the shift from primarily static content to more dynamic content improved the positioning of the FactNotFiction website in terms of search engine optimization (SEO). One of the primary ways that web designers ensure SEO is by regularly updating the content (Safko, 2012), and another important SEO technique involves linking other accounts into and out from the site. The more incoming and outgoing links, the higher the site will appear in relevant searches (Safko, 2012).
Fourth, it has been argued that millennials—i.e., youth/young adults who are “the first generation who don’t know life without the internet and personal tech devices” (Pollak, 2015, p. 1)—are particularly drawn to the shorter-form content that a platform such as Tumblr provides (Anderson & Rainie, 2012). Finally, the site redesign of FactNotFiction eliminated the original site’s potentially overwhelming main screen. With 31 topic tabs to choose from on the original site, it is likely that visitors who felt overwhelmed by the array of possible selections from which to choose instead opted to leave the site rather than make a topic selection (Schwartz, 2005). Overall, the relaunch of the FactNotFiction site solved many of the initial issues that likely contributed to overlooking or dismissing the original site and its valuable information among members of FactNotFiction’s primary the target audience of Mississippi youth/young adults (as evidenced by the original site’s high bounce rate, etc.).
Results of this case study and other emerging research suggest that to be effective, an online comprehensive sex education site for youth needs to meet a number of criteria. First, the site should be age-appropriate for the target audience and “positioned within the complexity of their real-life experiences” (Mak, Bastian, Grace, Aquilina, & Sweeting, 2012, p.199) to ensure that the site’s content has relevance for this unique demographic. Second, the site should be perceived by youth as a trustworthy online resource (Ghaddar, Valerio, & Garcia, 2012). Third, the site should be evaluated relatively quickly after its initial launch using available online analytic tools (e.g., Google Analytics, Facebook Insights, Bitly) to determine effectiveness. Fourth, the site’s developers should be responsive to the analytic results so adjustments to the website’s structure and format can be rapidly executed if necessary.
Fifth, the site should be designed to be mobile-enabled and easily disseminated across multiple media channels to maximize likes and repeat visitors and to minimize bounce rates. Sixth, the site should be designed to be dynamic, given that fresh content is integral to retaining youth on social media sites. Seventh, the site needs to be sustainably funded over the long-term in order to maintain the site and regularly update content. Finally, the site should be evaluated using different qualitative and survey methods so results can be triangulated for comparison in order to provide a more complete picture of youth’s motivations for seeking online comprehensive sex education in general, and what they like and dislike about the present site (Mak, Bastian, Grace, Aquilina, & Sweeting, 2012; McCarthy, Carswell, Murray, Free, Stevenson, & Bailey, 2012). These results have implications for others involved in designing, launching, and monitoring technology-based public health education and prevention efforts targeting youth and other hard to reach populations.
Discussion Questions and Activities
- Was FactNotFiction successful in reaching its primary target population of Mississippi youth seeking sexual and reproductive health information? Why or why not?
- What about social media helps bridge the gap for youth who may lack access to sexual and reproductive health information? Explain your position.
- Small group exercise: Consider the different social media platforms currently available: Facebook, Twitter, Tumblr, Instagram, Pinterest, etc. How would youth-oriented sexual and reproductive health information be presented differently on each of these platforms? Decide which social media tools or channels you would select and what kinds of youth-oriented sexual and reproductive health messages you would use for each platform.
- How would the implementation of a social media site to deliver sexual and reproductive health information to youth be different for different target audiences of youth, such as at-risk Young Men Who Have Sex with Men (YMSM) (CDC, 2015c) or adolescent girls in developing nations (Advocates for Youth, 2015b ; Hindin, Christiansen, & Ferguson, 2012)?
- In terms of eHealth literacy among youth, how have Internet sites changed the way youth seek and use sexual health information? Is the Internet an effective way to communicate sexual and reproductive health information to youth? Why or why not? What are potential pitfalls of using the Internet to communicate sexual and reproductive health information to youth? How might youth be trained to better evaluate whether the sexual and reproductive health information they receive via the Internet is reliable, accurate, and trustworthy?
- What are ‘best practices’ to evaluate the effectiveness of social media sites whose goal is to deliver sexual and reproductive health information to youth?
- Form two teams to debate the multiple changes that the FactNotFiction research group made to the FactNotFiction social media campaign. Each team should select one change that they feel is the primary reason that the FactNotFiction relaunch was more successful than the initial launch. Next, each team should rank—in order of perceived effectiveness—the remaining changes that were made. Present your results and reasoning to the other team. Was there another reason for the improved efficacy of the campaign that the authors did not address?
References
Advocates for Youth. (2015a). Sex education programs: Definitions & point-by-point comparison. Retrieved December 31, 2015, from http://www.advocatesforyouth.org/publications/publications-a-z/655-sex-education-programs-definitions-and-point-by-point-comparison
Advocates for Youth. (2015b). The sexual and reproductive health of adolescent girls in low and middle income countries. Retrieved December 31, 2015, from http://www.advocatesforyouth.org/publications/publications-a-z/2474-the-reproductive-and-sexual-health-of-adolescent-girls-in-low-and-middle-income-countries
Allard, S. (2013). We’ve tested the new Facebook Insights: Our in-depth review. Retrieved December 31, 2015, from http://www.wiselytics.com/blog/new-facebook-page-insights-our-in-depth-review/
Anderson, J. & Rainie, L. (2012). Millennials will benefit and suffer due to their hyperconnected lives. Pew Research Center. Retrieved December 31, 2015, from http://www.pewinternet.org/2012/02/29/millennials-will-benefit-and-suffer-due-to-their-hyperconnected-lives/
Beaulieu, L. J., & Gallardo, R. (2012). Mississippi broadband quick facts. Southern Rural Development Center, Mississippi State University. Retrieved December 31, 2015, from http://srdc.msstate.edu/news/files/brief6.pdf
Blue Fountain Media (BFM). (2013). What is behavioral targeting? Retrieved December 31, 2015, from http://www.bluefountainmedia.com/glossary/behavioral-targeting/
Boonstra, H. D. (2014). What is behind the declines in teen pregnancy rates? Guttmacher Policy Review, 17(3), 15-21.
Bull, S. S., Levine, D. K., Black, S. R., Schmiege, S. J., & Santelli, J. (2012). Social media-delivered sexual health intervention: A cluster randomized controlled trial. American Journal of Preventive Medicine, 43, 467-474.
Brewin, D., Koren, A., Morgan, B., Shipley, S., & Hardy, R. L. (2014). Behind closed doors: School nurses and sexual education. Journal of School Nursing, 30, 31-41.
Carpenter, K. M., Stoner, S. A., Mikko, A. N., Dhanak, L. P., & Parsons, J. T. (2010). Efficacy of a web-based intervention to reduce sexual risk in men who have sex with men. AIDS and Behavior, 14, 549-557.
Centers for Disease Control and Prevention (CDC). (2015a). 2013 sexually transmitted disease surveillance. U.S. Department of Health and Human Services. Retrieved December 31, 2015, from http://www.cdc.gov/std/stats13/adol.htm
CDC. (2015b). Mississippi 2013 and United States 2013 results: High school youth risk behavior survey. Retrieved December 31, 2015, from http://nccd.cdc.gov/youthonline/App/Results.aspx?LID=MS
CDC. (2015c). The Young Men Who Have Sex with Men (YMSM) Project: Reducing the risk of HIV/STD infection. Retrieved December 31, 2015, from http://www.cdc.gov/healthyyouth/disparities/ymsm/
CDC. (2012). HIV, other STD, and teen pregnancy prevention and Mississippi students. U.S. Department of Health and Human Services. Retrieved December 31, 2015, from http://www.cdc.gov/healthyyouth/yrbs/pdf/hiv/ms_hiv_combo.pdf
Dunne, A., McIntosh, J., & Mallory, D. (2014). Adolescents, sexually transmitted infections, and education using social media: A review of the literature. The Journal for Nurse Practitioners, 10(6), 401-408.
Eisenberg, M. E., Madsen, N., Oliphant, J. A., & Sieving, R. E. (2013). Barriers to providing the sexuality education that teachers believe students need. Journal of School Health, 83, 335-342.
Ghaddar, S. F., Valerio, M. A., & Garcia, C. (2012). Adolescent health literacy: The importance of credible sources for online health information. Journal of School Health, 82, 28-36.
Goldman, J. D. (2011). An exploration in health education of an integrated theoretical basis for sexuality education pedagogies for young people. Health Education Research, 26, 526-541.
Goodkind, S., Schelbe, L., Joseph, A. A., Beers, D. E., & Pinsky, S. L. (2013). Providing new opportunities or reinforcing old stereotypes? Perceptions and experiences of single-sex public education. Children and Youth Services Review, 35, 1174-1181.
Google Analytics. (2015a). Introduction to Google Analytics. Retrieved December 31, 2015, from http://support.google.com/analytics/answer/1008065?hl=en&ref_topic=1008008
Google Analytics. (2015b). Content: Bounce rate. Retrieved December 31, 2015, from http://support.google.com/analytics/answer/1009409?hl=en
Halpern, D. F., Eliot, L., Bigler, R.S., Fabes, R.A., Hanish, L.D., Hyde, J., Liben, L.S., & Martin, C. L. (2011). Education. The pseudoscience of single-sex schooling. Science, 333, 1706-1707.
Hindin, M. J., Christiansen, C. S., & Ferguson, B. J. (2013). Setting research priorities for adolescent sexual and reproductive health in low- and middle-income countries. Bulletin of the World Health Organization, 91, 10-18. Retrieved December 31, 2015, from http://www.who.int/bulletin/volumes/91/1/12-107565/en/
Jones, K., Eathington, P., Baldwin, K., & Sipsma, H. (2014). The impact of health education transmitted via social media or text messaging on adolescent and young adult risky sexual behavior: A systematic review of the literature. Sexually Transmitted Diseases, 41(7), 413-419.
Jones, R. K., & Biddlecom, A. E. (2011). Is the Internet filling the sexual health information gap for teens? An exploratory study. Journal of Health Communication, 16, 112-123.
Kelly, K. (2015). What is bounce rate? Avoid common pitfalls. Blast Analytics & Marketing. Retrieved December 31, 2015, from http://www.blastam.com/blog/index.php/2012/02/what-is-bounce-rate
Kelsey, M., & Layzer, J. (2014). Implementing three evidence-based program models: Early lessons from the Teen Pregnancy Prevention Replication Study. Journal of Adolescent Health, 54(3 Suppl), S45-S52.
Kempner, M. (2014). Tucson students skipping sex ed, restrictive policy may be to blame. RH Reality Check. Retrieved December 31, 2015, from http://rhrealitycheck.org/article/2014/05/01/tucson-students-skipping-sex-ed-restrictive-policy-may-blame/
Kohler, P. K., Manhart, L. E., & Lafferty, W. E. (2008). Abstinence-only and comprehensive sex education and the initiation of sexual activity and teen pregnancy. Journal of Adolescent Health, 42, 344-351.
Lenhart, A. (2015). Teens, social media & technology overview 2015. Pew Research Center. Retrieved December 31, 2015, from http://www.pewinternet.org/files/2015/04/PI_TeensandTech_Update2015_0409151.pdf
Madden, M., Lenhart, A., Duggan, M., Cortesi, S., & Gasser, U. (2013). Teens and technology 2013. Pew Research Center. Retrieved December 31, 2015, from http://www.pewinternet.org/files/oldmedia//Files/Reports/2013/PIP_TeensandTechnology2013.pdf
Mak, D. B., Bastian, L., Grace, J., Aquilina, H., & Sweeting, J. (2012). Evaluation of a sexual health and blood-borne virus health education website for youth. Health Promotion Journal of Australia, 23, 194-200.
Marsac, M. L., Kassam-Adams, N., Hildenbrand, A. K., Kohser, K. L., & Winston, F. K. (2011). After the injury: Initial evaluation of a web-based intervention for parents of injured children. Health Education Research, 26, 1-12.
McCarthy, O., Carswell, K., Murray, E., Free, C., Stevenson, F., & Bailey, J. V. (2012). What young people want from a sexual health website: Design and development of Sexunzipped. Journal of Medical Internet Research, 14, e127.
McKee, C., Ragsdale, K., & Southward, L. H. (2014). What do parents in Mississippi really think about sex education in school?: Results of a state-wide survey. Journal of Health Disparities Research and Practice, 7(1), 97-119.
Melaugh, S. (2014). Web stats: Alternatives to Google Analytics. Retrieved December 31, 2015, from http://imimpact.com/web-stats-alternatives-to-google-analytics/
Miedema, E. A., Maxwell, C., & Aggleton, P. (2011). Education about HIV/AIDS–Theoretical underpinnings for a practical response. Health Education Research, 26, 516-525.
Mississippi State Legislature. (2011). House Bill 999 (as sent to Governor). Retrieved December 31, 2015, from http://billstatus.ls.state.ms.us/documents/2011/pdf/HB/0900-0999/HB0999SG.pdf
National Campaign to Prevent Teen and Unplanned Pregnancy (NCPTUP). (2015a). Fast facts: How does the United States compare? Retrieved December 31, 2015, from https://thenationalcampaign.org/resource/fast-facts-how-does-united-states-compare
NCPTUP. (2015b). National & state data. Retrieved December 31, 2015, from http://thenationalcampaign.org/data/landing
National Conference of State Legislators (NCSL). (2015). State policies on sex education in schools. Retrieved December 31, 2015, from http://www.ncsl.org/issues-research/health/state-policies-on-sex-education-in-schools.aspx
Nsoesie, E. (2014). Digital disease detection: Using social media to predict flu trends. Retrieved December 31, 2015, from http://www.healthmap.org/site/diseasedaily/article/digital-disease-detection-using-social-media-predict-flu-trends-31114
Ott, M. A., Rouse, M., Resseguie, J., Smith, H., & Woodcox, S. (2011). Community-level successes and challenges to implementing adolescent sex education programs. Maternal and Child Health Journal, 15, 169-177.
Owyang J. (2007). Thinking bigger, past the limitations of web analytics. Retrieved December 31, 2015, from http://www.web-strategist.com/blog/2007/07/26/web-analytics-is-limited/
Paek, H. J., & Hove, T. (2012). Social cognitive factors and perceived social influences that improve adolescent eHealth literacy. Health Communication, 27, 727-737.
Pettus, E. W., & Amy, J. (2012). More than half of Mississippi school districts choose abstinence-only sex education curriculum (with list). The Mississippi Press. Retrieved December 31, 2015, from
http://blog.gulflive.com/mississippi-press-news/2012/07/more_than_half_of_mississippi.html
Pollak, L. (2015). What is a millennial? Everything you’ve always wanted to know but were afraid to ask. Retrieved December 31, 2015, from http://www.lindseypollak.com/what-is-a-millennial-everything-youve-always-wanted-to-know-but-were-afraid-to-ask/
Ragsdale, K., & Sutton, L. (2012). Policy scan: Risk factors and health status of Mississippi youth, 2012. Starkville, MS: Social Science Research Center, Mississippi State University.
Safko, L. (2012). The social media bible: Tactics, tools, and strategies for business success (3rd ed.). Hoboken, NJ: Wiley.
Santelli, J.,& Kirby, D. (2010). State policy effects on teen fertility and evidence-based policies. Journal of Adolescent Health, 46(6), 515-516.
Santelli, J., Ott, M. A., Lyon, M., Rogers, J., Summers, D., & Schleifer, R. (2006). Abstinence and abstinence-only education: a review of U.S. policies and programs. Journal of Adolescent Health, 38(1), 72-81.
Sexuality Information and Education Council of the United States (SIECUS). (2014). Sexuality education in Mississippi: Progress in the magnolia state. Retrieved December 31, 2015, from http://www.siecus.org/document/docWindow.cfm?fuseaction=document.viewDocument&documentid=201&documentFormatId=257
SIECUS. (2009). What the research says…Comprehensive sex education. Retrieved December 31, 2015, from http://www.siecus.org/_data/global/images/What%20the%20Research%20Says-CSE-1.pdf
Simon, L., & Daneback, K. (2013). Adolescents’ use of the Internet for sex education: A thematic and critical review of the literature. International Journal of Sexual Health, 25(4), 305-319.
Smith, C. (2013). Tumblr offers advertisers amajor advantage: Young users, who spend tons of time on the site. Business Insider. Retrieved December 31, 2015, from http://www.businessinsider.com/tumblr-and-social-media-demographics-2013-12
Stanger-Hall, K. F., & Hall, D. W. (2011). Abstinence-only education and teen pregnancy rates: Why we need comprehensive sex education in the U.S. PLOS Medicine, 4, e275.
Schwartz, B. (2005). The paradox of choice: Why more is less. New York City, NY: Harper Perennial.
Smith, A. (2015). US smartphone use in 2015. Pew Research Center. Retrieved December 31, 2015, from http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/
Statista. (2015). Smartphone penetration in the United States from 2008 to 2014 (in percent of new handset sales). Retrieved December 31, 2015, from http://www.statista.com/statistics/218529/us-martphone-penetration-since-2008/
Tortolero, S. R., Johnson, K., Peskin, M., Cuccaro, P.M., Markham, C., Hernandez, B. F., Addy, R. C., Shegog, R., & Li, D. H. (2011). Dispelling the myth: what parents really think about sex education in schools. Journal of Applied Research on Child, 2(2), 1-19.
U.S. Department of Health and Human Services. (2014). Mississippi adolescent reproductive health facts. Office of Adolescent Health. Retrieved December 31, 2015, from http://www.hhs.gov/ash/oah/adolescent-health-topics/reproductive-health/states/ms.html#footnote-1
Walton, L. R., Seitz, H. H., & Ragsdale, K. (2012). Strategic use of YouTube during a national public health crisis: The CDC’s response to the 2009 H1N1 flu epidemic. Case Studies in Strategic Communication, 1, 25-37. Retrieved December 31, 2015, from http://cssc.uscannenberg.org/wp-content/uploads/2013/10/v1art3.pdf
KATHLEEN RAGSDALE, PhD, MA, is an associate research professor at the Mississippi State University Social Science Research Center. She is an applied medical anthropologist who is currently conducting mixed method research on how new media/electronic technologies can be harnessed to address health disparities among minority and vulnerable populations, with a particular focus on high risk behavior prevention among rural and at-risk youth. Email: Kathleen.Ragsdale[at]ssrc.msstate.edu.
SYDNEY K. HARPER, MS, CHES, is the Program Coordinator for the Southern Alabama Area Health Education Center (SAAHEC). She is a Certified Health Education Specialist who currently leads the SAAHEC Community Based Student Education and Health Careers Preparation and Promotion programs. Email: sydneykharper[at]gmail.com.
SHEEJI KATHURIA, MLIS, is an Assistant Professor and the Social Sciences Librarian at the Mississippi State University Libraries. Her research interests include reference services assessment, scholarly communication, and social media. Email: skathuria[at]library.msstate.edu.
JAMIE H. BARDWELL, MPP, is the deputy director of the Women’s Foundation of Mississippi. Jamie leads the grantmaking and advocacy programs of the Women’s Foundation and is particularly interested in evidence-based strategies to reduce teen and unplanned pregnancies. Email: jamie[at]womensfoundationms.org.
CAROL B. PENICK, founding Executive Director of the Women’s Foundation of Mississippi, has led the Foundation in its growth from a small program at the Community Foundation of Greater Jackson to an independent statewide nonprofit. Since the launch as the Women’s Foundation of Mississippi in 2009, Penick’s vision for helping women in Mississippi thrive has grown the grantmaking base from $68,000 in year one to approximately $1 million in 2016, and has brought $4.5 million of investment into the state.
MICHAEL BREAZEALE, PhD, is an assistant professor of marketing at Mississippi State University. His mixed-methods research focuses on branding and social media, and he is currently conducting research on the branding practices of violent extremist organizations, consumers’ affective responses to brands, and retail atmospherics. Email: mbreazeale[at]business.msstate.edu.
Acknowledgments
FactNotFiction is supported by the Mississippi State Department of Health (website development) and an anonymous donor (media campaign). Preparation of this manuscript is supported by the Social Science Research Center, Division of Agriculture, Forestry and Veterinary Medicine of Mississippi State University and by the Women’s Foundation of Mississippi. This manuscript was informed by research conducted by the first author funded by My Brother’s Keeper Inc. with support from the Centers for Disease Control and Prevention (Cooperative Agreement Number 1U58DP003711). We gratefully acknowledge Kina L. Johnson of the Mississippi State Department of Health and Abby Rosenstein of Advocates for Youth for their invaluable input into FactNotFiction. We also gratefully acknowledge the FactNotFiction Youth Advisory Council members and Kristine Jacobs, Tom Allin, Anne-Lauren Fratesi, Josh Schooler, and Wes Williams of The Ramey Agency for their important contributions to FactNotFiction.
Editorial history
Received June 5, 2015
Revised December 31, 2015
Accepted December 31, 2015
Published December 31, 2015
Handled by editor; no conflicts of interest